E LOG of Ruchitha
60 year old woman, who previously worked as a coolie presented with the chief complains of
Pain abdomen since 1 :30pm yesterday
Followed by 2 episodes of vomitings
She attained menarche at 15 yrs age and she got married to a daily laborer. She has given birth to 8 children ( 4 daughters , 4 sons).
18 years back she got dyspneic on a cold winter night when she was rushed to a local hospital and was put on budecort and ashtalin as told by the attendant. Ever since then she has been experiencing dyspnea and cough during winters and has everytime been using levosalbutamol and budecort inhaler.
15 years back she got admitted in a hospital with fever when she was told that she was diabetic and was put on oral medications which she has been using regularly since then.
She has been occasionally consuming alcohol around 90 ml of whiskey once a month. 4 days back she consumed 90ml of whiskey when all her family got together and also tells she ate home made chicken last night. She presented to us yesterday with the complains of pain abdomen since 1:30pm which is diffuse though it was more in her right hypochondriac which was aggravated on food consumption, which releaved on leaning forward. After 1 hour of onset of her pain abdomen she 2 episodes of vomitings which were non projectile, non bilious and non blood tinged, containing food content.
She gives no history of fever, loose stools, cough,
No history of intake of outside or canned food
She gives no complains of myalgias, sore throat, fever or neck pain, fatigue, body aches.
She is diabetic since 15 yrs and obese,
She had no pallor, lymphadenopathy, cyanosis, clubbing, icterus


On initial assessment, her temperature was 98.6 F, PR was 99bpm with a BP of 130/70mmhg, respiratory rate of 19 cycles per minute and she was maintaining saturation at 99%, her blood glucose level was 187 mg/dl.
On examination, her abdomen was soft on palpation, there was diffuse tenderness and she said she experienced more pain when her right hypochondrium was palpated, bowel sounds were active throughout the abdomen. Her lungs were clear on auscultation and on Auscultation of the heart, S1 and s2 were heard.
Her oropharyngeal examination was normal
There was no lymphadenopathy
Since morning she has been febrile, her temp is 102 and also has had 3 episodes of loose stools, small in quantity, mucoid, non blood tinged, no tenesmus
CBP:
Hb 10.8
TLC 13,000
Neutrophil :83
Lymphocytes :11
Normocytic normochromic with Neutrophil leucocytosis
CUE:
Albumin (negative )
Sugar ++
Bilesalts and bile pigments (-)
Epithelial cells2-3
Puscells 2-3
RFT:
Urea 42
Creatinin 1.0
Uric acid 3.8
Calcium 10.2
Phosphorus 2.8
Potassium 3.4
Chloride 95
Sodium 139
LFT
Total bilirubin 1.77
Direct bilirubin 0.59
AST 62
Alt 36
Alkaline phosphatase 209
A/g ratio 1.36
Total protein 6.4
Albumin 3.9
Serum amylase 705IU /L
Serum lipase 129IU/L
USG- GB wall edema
No cholelithiasisi /percholecytic fluid
Body of pancreas homgenous hetero cholic
17 mm fatty uninfiltration
B/L Grade 1 RPD
Grade 1 fatty liver disease
Ecg



Treatment :
1. NBM
2.IVF 20NS, 10RL continuous infusion. 100ml/hr
3.INJ PAN 40 mg /IV/OD
4. INJ ZOFER 4mg/IV/OD
5.INJ TRAMADOL 1 AMP in 100ml NS / iv/BD
6.STRICT I/0 Charting
7. Temperature charting
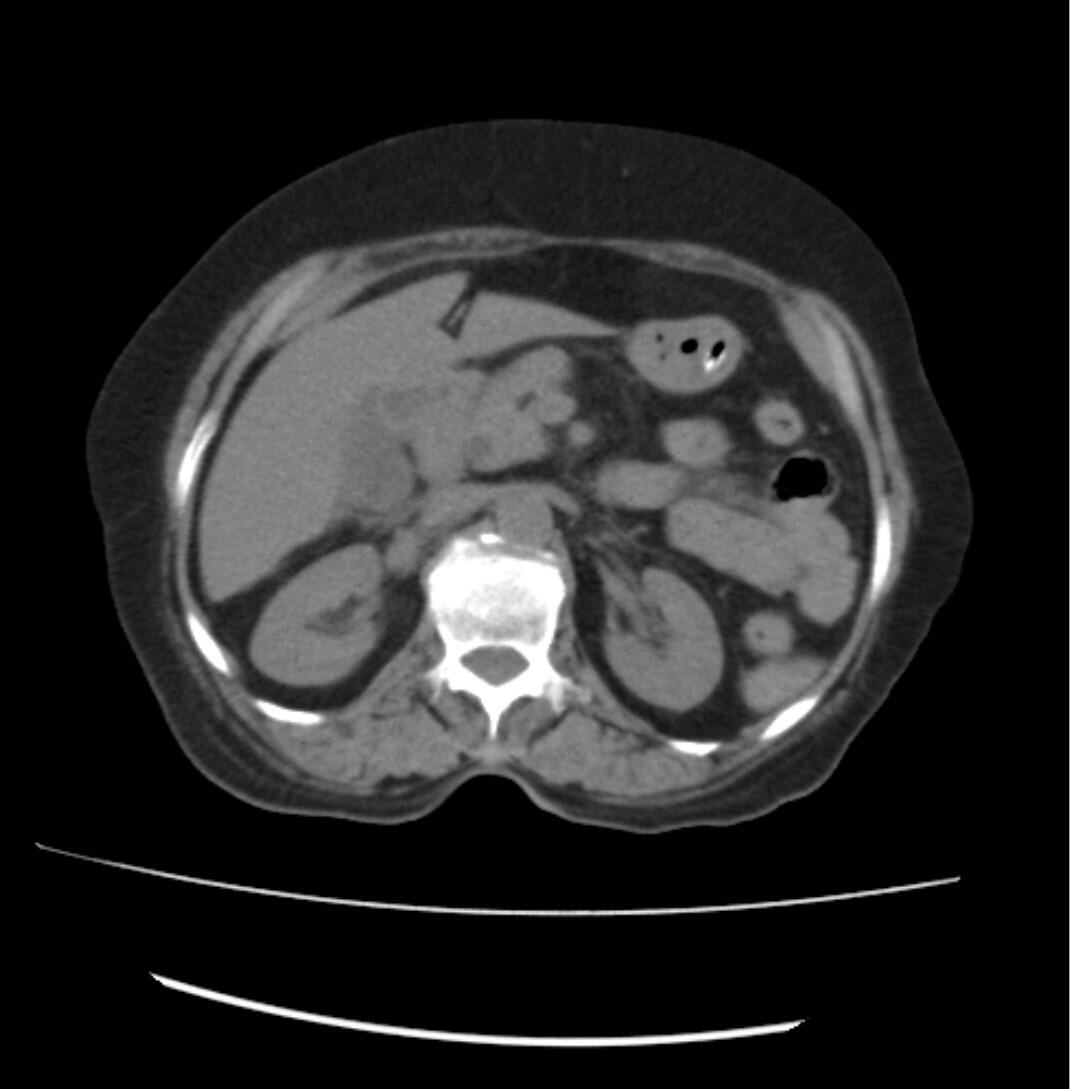
CECT





A sonogram for acute acalculous cholecystitis may be considered highly suggestive of the diagnosis with two of the following major criteria, or one major and two minor criteria fulfilled
major criteria:
gallbladder wall thickness >3 mm
wall striation
pericholecystic fluid
sonographic Murphy sign
intramural gas
mucosal sloughing
minor criteria:
echogenic bile or sludge in the lumen
transverse diameter >5 cm
https://radiopaedia.org/articles/acute-acalculous-cholecystitis
PROBABLE DIAGNOSIS :
Acute cholecystitis ?secondary to viral etiology.
Known case of type 2 diabetes mellitus since 15 years



{kind=link}
{kind=link}
{kind=link}
Comments
Post a Comment